Quick version
Calcium score is a rapid computed tomography scan of the coronary arteries that measures the amount of calcification and provides a more individual assessment of the risk of future cardiovascular disease. The examination is particularly valuable for people without symptoms where the traditional risk assessment is uncertain, for example in the case of elevated blood lipids or heredity. A score of 0 is usually a reassuring finding, while higher values indicate an increased incidence of atherosclerosis and can influence decisions about preventive treatment. At the same time, calcium score is a complement to – not a replacement for – assessment of blood lipids, blood pressure, diabetes, lifestyle and other established risk factors.
Feeling healthy is not the same as being free from cardiovascular disease. Atherosclerosis often develops silently for many years, without clear symptoms, until it manifests itself as angina, heart attack or stroke. This is precisely why the calcium score is of great interest, as the examination can detect calcifications in the coronary arteries of the heart before the disease has had time to cause problems. For many, it is a way to get a more precise picture of their future cardiovascular risk – especially when blood lipids, blood pressure, heredity or other risk factors provide an uncertain overall picture.
What does calcium score mean – a test to assess cardiovascular risk?
Calcium score, also called coronary calcium score or CAC score, is a computed tomography of the heartthat measures the amount of calcium in the coronary arteries. Calcium in the coronary arteries is a marker for atherosclerosis, i.e. atherosclerosis. The more calcification that is seen, the greater the likelihood that there is atherosclerotic disease and the higher the future risk of cardiovascular events.
This examination is performed without contrast medium, usually takes only a few minutes and requires no recovery time. The result is usually given as an Agatston score, where higher values indicate a greater amount of calcium and a higher risk. A score of 0 indicates that no calcification could be detected at the time of the examination, while higher levels are divided into minimal, mild, moderate or extensive calcification.
How does the calcium score work and what does the examination show?
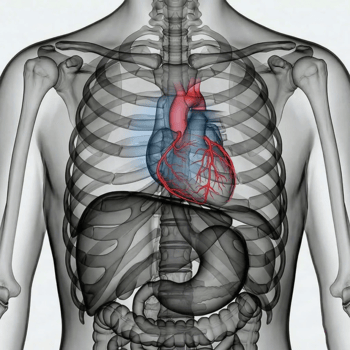
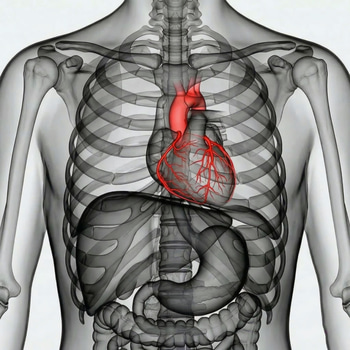
The coronary arteries supply the heart muscle with oxygen-rich blood. In atherosclerosis, plaque builds up in the vessel wall. Some of these plaques contain calcium, and it is precisely this calcium that can be detected with CT. Calcium score does not just show cholesterol levels or blood pressure on paper, but provides an image of whether risk factors have already had time to affect the vessels biologically.
It is important to understand that the examination measures calcified plaque burden, not how narrow a vessel is in real time. Therefore, calcium score alone cannot be used to determine exactly whether a certain narrowing is present or how pronounced it is. In case of chest pain or suspected angina, other investigations are often needed, such as coronary CT with contrast or other cardiac investigations.
Common risk levels are usually described as follows:
0: no calcification detected
1–10: minimal calcification
11–100: mild calcification
101–400: moderate calcification
Over 400: extensive calcification
However, this does not mean that everyone with a score of 0 is “completely protected”, or that everyone with high values will get a myocardial infarction. The result must always be interpreted together with age, gender, blood lipids, blood pressure, diabetes, smoking, family history and sometimes also other markers such as lipoprotein(a).
When can the calcium score be valuable in assessing cardiovascular risk?
The calcium score is mainly used in primary prevention, i.e. in people who have not yet had a heart attack, stroke or other established atherosclerotic cardiovascular disease. The greatest benefit is often seen when the usual risk assessment ends up in a borderline state – for example, when wondering whether a person should start statin treatment or intensify their prevention. European guidelines state that CT for coronary calcium can be considered in asymptomatic adults at moderate risk to improve risk assessment.
Examples of situations where the examination may be particularly relevant:
You have elevated LDL cholesterol but are unsure of the urgency of treatment
You have a family history of early cardiovascular disease
You have several risk factors, such as high blood pressure, abdominal obesity, prediabetes or smoking
Your overall risk according to calculators is perceived as difficult to interpret
You want to get a more concrete picture of whether risk factors have already left their mark on the vessels
There are also situations where the calcium score is not the right first choice. In people with known cardiovascular disease, the examination rarely adds anything decisive, since the risk is already elevated and prevention should already be clear. It is also advised not to routinely order calcium scores in patients with established atherosclerotic disease.
Nor should calcium scores be seen as a quick shortcut to diagnosis in the presence of current symptoms, such as new chest pain or shortness of breath on exertion. In such cases, a symptom-based medical assessment is required instead.
How is the answer interpreted – and what does a score of 0, 100 or 400 mean?
A common question is whether a calcium score of 0 means that there is no risk of cardiovascular disease. The answer is no. However, the risk of cardiac events in the short and medium term is often lower compared to people who have demonstrated calcification in the coronary arteries. A calcium score of 0 is therefore generally considered a reassuring finding, especially in people without symptoms who are undergoing a preventive cardiovascular assessment. At the same time, soft, non-calcified plaques can still occur, and other risk factors continue to have a significant impact on the overall risk.
If the score is 1–100, there is evidence of early to mild atherosclerosis. The focus then often becomes on reviewing lifestyle and assessing the need for drug treatment, especially if other risk factors are present at the same time. At 101–400, the finding indicates a clearer plaque burden and a higher future risk. At over 400, the calcification is extensive, and the likelihood of significant atherosclerotic disease is clearly higher.
So what is important is not just the number itself, but what it means for the next step. A calcium score can influence decisions about:
need for statin therapy
how aggressively LDL cholesterol should be lowered
the importance of treating blood pressure, diabetes or prediabetes
motivation to quit smoking, exercise and control weight
need for further medical assessment depending on symptoms and overall risk profile
What are the benefits, limitations and risks of the calcium score?
The major advantage of the calcium score is that the examination can provide a more individualized risk assessment than traditional risk factors alone. Two people can have the same cholesterol and blood pressure, but completely different degrees of actual atherosclerosis. Therefore, the method is often used to “reclassify” risk – from uncertain to more clearly low or high risk.
Other advantages are that the test:
is non-invasive
does not require contrast media
is quick
is usually painless
can strengthen motivation for preventive treatment when the result becomes concrete
However, the examination also has limitations. It does not find all types of plaque, especially not purely non-calcified ones. It is also not designed to explain acute symptoms. A high value indicates that atherosclerosis is present, but not exactly where a critical narrowing is located or whether a plaque is unstable.
There are also certain disadvantages and risks:
ionizing radiation, even if the dose is relatively low
risk of over-examination after a high finding
concern in people who receive a different result
risk of false security if a score of 0 is misinterpreted as no action is needed
What can you do yourself if your cardiovascular risk needs to be assessed?
For most people, a wise cardiovascular assessment does not begin with CT, but with mapping the factors that actually drive risk over time. These include:
blood sugar or HbA1c
smoking
waist circumference, weight and physical activity
heredity for premature cardiovascular disease
sometimes complementary markers such as lipoprotein(a)
Calcium score is therefore best seen as a complement, not as a replacement for classic risk assessment, lifestyle changes or medical treatment. The big gain occurs when the result leads to the right action at the right time.