Quick version
A cyst in the pancreas is often discovered by chance during diagnostic imaging examinations and does not automatically mean cancer. Most cysts are benign and never cause any problems, but certain types may have an increased risk of developing into cancer and therefore need to be followed up or treated. The investigation is based primarily on magnetic resonance imaging, computed tomography and, if necessary, endoscopic ultrasound. Treatment is adapted to the type of cyst, size, any symptoms and individual cancer risk.
Changes in the pancreas are often discovered by chance during examinations performed for other reasons. Perhaps a CT scan has been performed due to gallstones, kidney stones or back pain, and the report suddenly mentions a pancreatic cyst. For many, such news raises concerns, not least because the pancreas is often associated with serious diseases.
However, it is important to know that a pancreatic cyst does not automatically mean cancer. Many cysts are benign, cause no symptoms and never need to be treated. The most important thing is to determine what type of cyst it is, whether it causes problems and whether it has characteristics that warrant further investigation or regular follow-up.
What is a pancreatic cyst?
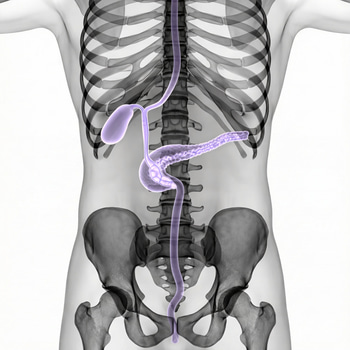
A pancreatic cyst is a fluid-filled change in or on the pancreas, the organ that lies behind the stomach and helps the body with both digestion and blood sugar regulation. Many are discovered by chance during ultrasound, computed tomography or magnetic resonance imaging (MRI) which is done for completely different reasons.
There are several different types. They can be roughly divided into two main groups: pseudocysts, which most often occur after inflammation of the pancreas, and cystic tumors, some of which are benign while others may be precursors to cancer.
Common cystic tumor types are IPMN, serous cystadenoma and mucinous cystic neoplasia. For those who are first diagnosed, this division is more important than the size itself, since the risk and follow-up differ clearly between different cyst types.
Different types of pancreatic cysts
A pseudocyst is not actually a “true” cyst with a regular cyst wall. It consists of fluid that has collected after the pancreas has been inflamed or damaged, for example after acute pancreatitis, gallstones, high alcohol consumption or trauma to the abdomen.
IPMN is a type of cyst that originates from the pancreatic duct system and forms mucus. It is important to know because some IPMN changes can progress to cancer over time, especially if the main duct is affected or if other risk factors are present.
Serous cystadenoma is usually benign and has a very low risk of cancer. Mucinous cystic neoplasia is a less common type of cyst that is assessed with particular caution, as it has an increased risk of containing precancerous or, in some cases, cancer.
For the patient, the practical question is therefore not just “do I have a cyst?” but rather: “what kind of cyst is it, and does it need to be followed?”. This is also why the doctor often recommends a new MRI scan or endoscopic ultrasound instead of giving a definitive answer right away.
What symptoms can you get with a pancreatic cyst?
Many people have no symptoms at all. This is especially true for small cysts that are discovered by chance and that never affect either digestion or general condition.
When symptoms occur, they often involve persistent pain high in the abdomen, sometimes radiating to the back. You may also feel full early, feel sick, vomit or lose weight without a clear explanation.
Some people seek medical attention because their skin or the whites of their eyes have turned yellow. This may be because a cyst is pressing on the bile ducts, especially if the change is in the head of the pancreas. Jaundice is an alarm symptom that should always be assessed urgently.
In the case of pseudocysts, the picture is often more dramatic. In this case, there is often a recent or previous episode of pancreatitis in the background, with severe abdominal pain, nausea and sometimes fever. If a pseudocyst becomes infected, bleeds or ruptures, the condition can become acute.
Seek medical attention quickly if:
new or worsening upper abdominal pain
jaundice
fever with abdominal pain
repeated vomiting
rapid unexplained weight loss
bloody vomiting or signs of internal bleeding in a known pseudocyst.
How is a pancreatic cyst diagnosed?
The first step for a diagnosis is almost always imaging. Magnetic camera with MRCP is often used to assess the size of the cyst, its contents and whether it is in contact with the pancreatic duct system. Computed tomography can also provide valuable information, especially if you also want to assess inflammation, calcifications or other changes in the abdomen.
If the cyst is larger, looks suspicious or has so-called risk signs, you can proceed with endoscopic ultrasound, often abbreviated EUS. Then a thin tube is passed through the mouth to the stomach and duodenum so that the doctor can examine the pancreas very closely and sometimes take samples from the cyst fluid with a thin needle.
What the doctor is especially looking for is things that increase the likelihood of more serious changes. Examples are growth over time, nodules in the cyst wall, thickened wall, dilated main pancreatic duct, recurrent pancreatitis, elevated CA 19-9 or jaundice.
That is why follow-up may be needed even when cancer is not suspected here and now. The aim is to detect changes in time, before they become dangerous, and at the same time avoid unnecessary surgery in people with low risk.
Treatment and follow-up of pancreatic cysts
Treatment depends entirely on the type of cyst and risk profile. Most cysts do not require surgery, but are followed with imaging diagnostics for a shorter or longer period of time. This is especially true for small cysts without symptoms and without worrying findings.
Surgery is considered when the cyst has clear high-risk signs or when it is typically assessed to have significant potential to develop into cancer. Since pancreatic surgery is a major procedure with a significant risk of complications, the benefit of surgery is always weighed against the patient's age, other diseases and probable risk of cancer.
Pseudocysts are treated differently from other types of pancreatic cysts. Many pseudocysts decrease in size or disappear on their own over time and therefore do not require treatment. However, if a pseudocyst is large or causes symptoms, such as pain, infection, bleeding, or blockage in the gastrointestinal tract or bile ducts, it may need to be drained. This is usually done endoscopically, but in some cases through the skin or, more rarely, with surgery. At the same time, it is important to investigate and treat the underlying cause, usually pancreatitis.
When should blood tests and other warning signs be taken seriously?
A pancreatic cyst is not visible in regular blood tests, and there is no simple laboratory test that alone can determine whether a cyst is harmless or not. However, blood tests can provide important clues about how the pancreas and surrounding organs are doing, for example liver values in case of biliary tract involvement, inflammation samples in case of infection and glucose or HbA1c in case of blood sugar effects.
This is a common question in everyday life: “If my cyst was discovered by chance and I feel fine, do I still need to worry about my values?” The answer is often yes, because the pancreas is central to both metabolism and digestion. A new change in blood sugar, unexplained weight loss or liver effects can provide important supplementary information when following a cyst over time.
A pancreatic cyst is therefore not a diagnosis with a single answer, but a finding that must be placed in the right context. What makes the biggest difference is not to react the fastest, but to distinguish low risk from high risk with the right combination of imaging diagnostics, medical assessment and follow-up over time.