Quick version
Sarcopenia is a gradual loss of muscle strength and muscle mass that impairs balance and increases the risk of falls, even in people of normal weight. To investigate the condition, a DEXA X-ray is used to measure bone density and muscle mass, but the results must always be supplemented with physical function tests. When muscle loss coincides with osteoporosis (osteosarcopenia), the risk of fractures increases dramatically. The most effective treatment is progressive strength training combined with an increased protein intake of approximately 1.0–1.5 grams per kilogram of body weight per day.
Sarcopenia is rarely noticeable overnight. It often comes on insidiously: stairs feel heavier, balance becomes worse, you have less energy when walking and everyday lifting suddenly becomes strenuous. At the same time, bone density can decrease without any obvious symptoms at all – until a fall leads to a fracture. DEXA can provide valuable information about both bone mineral density and body composition, but the results always need to be interpreted in their medical context.
What is sarcopenia and how does a DEXA examination work?
Sarcopenia means that you have lost muscle strength and, if the diagnosis is confirmed, also muscle mass. Reduced muscle strength is the first and most important sign, while low muscle mass is used to confirm the diagnosis. When physical function is also clearly impaired, we speak of severe sarcopenia. This is important, as many people believe that sarcopenia is just about “too little muscle”, when in practice it is also about how the muscles function in everyday life.
DEXA, or dual-energy X-ray absorptiometry, is the established method for measuring bone density and is also used to analyze body composition, such as fat mass and muscle mass. For bone density, DEXA is considered the reference method in clinical practice, especially for the hip and lower back. For body composition, the same technique can estimate, among other things, appendicular lean mass, i.e. the muscle mass found in the arms and legs.
What is sarcopenia and why is it related to bone density?
Sarcopenia is a progressive condition in which muscle strength and muscle mass decrease, usually with increasing age. But age is not the only cause. Physical inactivity, insufficient protein intake, illness, inflammation, hormonal changes, underweight and long-term treatment with certain medications – for example glucocorticoids – can also contribute.
Muscles and skeleton influence each other biologically and mechanically. Strong muscles put a beneficial load on the skeleton and help maintain bone strength. When muscle strength decreases, the risk of falls also increases. Therefore, the combination of low muscle mass, reduced strength and low bone density can be particularly unfavorable. In the clinic, osteosarcopenia is sometimes referred to as osteosarcopenia when osteoporos or low bone density occurs together with sarcopenia. This combination is linked to a higher risk of functional impairment, falls and fractures.
There are several common concerns about how these conditions manifest themselves in everyday life, not least regarding body weight and diffuse symptoms. Many are surprised that you can actually suffer from sarcopenia even if the scale shows a completely normal weight, or even overweight. This is because body composition may be altered with a hidden lack of muscle mass or reduced muscle strength. Similarly, low bone density, such as in osteopenia or osteoporosis, rarely gives any clear warning signs or symptoms at all – it is often only discovered when a fracture occurs. It is also important to distinguish between general fatigue and sarcopenia, although fatigue itself can have many different causes, you should be extra careful if it occurs together with noticeable muscle weakness, poor balance and reduced physical strength. In those cases, there are good reasons to go further and investigate both muscle function and bone density.
How does a DEXA examination for bone density and muscle mass work?
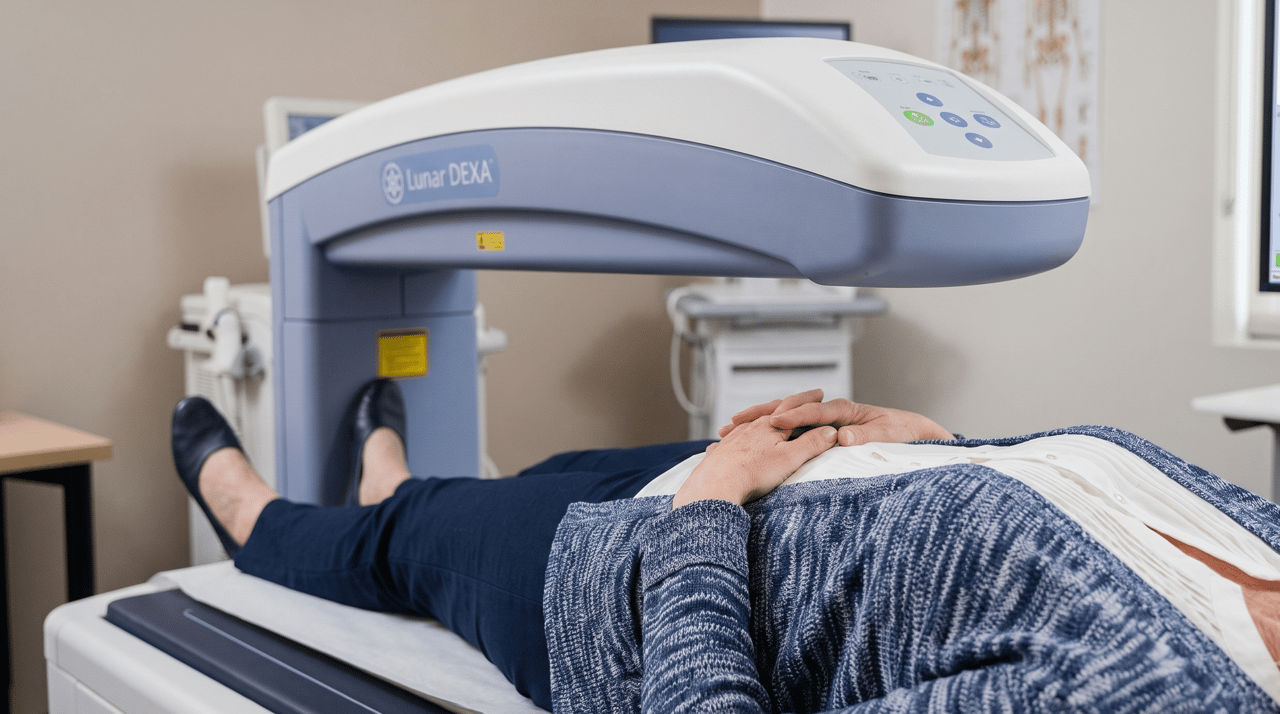
A DEXA scan is quick, painless and involves a low radiation dose. When measuring bone density, the hip and lower back are most often examined, as these areas provide important information about fracture risk and are used in established diagnostic criteria. DEXA is also used in many guidelines because the method has a strong link to future fracture risk.
When DEXA is used for body composition, it can estimate:
total fat mass
total lean mass
appendicular lean mass in arms and legs
sometimes indices that relate muscle mass to height, such as ALMI or ASMI
However, it is important to understand the limitations. DEXA does not measure muscle strength directly, and it cannot diagnose sarcopenia on its own. This requires that function is also assessed, for example through:
handgrip strength
chair rise test
gait speed
other standardized functional assessments
This means that a DEXA response should be interpreted together with clinical data. For example, a person may have relatively preserved muscle mass but still have low strength. Conversely, someone may have low muscle mass on DEXA but still function well in everyday life. The diagnosis must therefore be based on the whole.
When should bone density and muscle mass be checked?
There is no single rule that fits everyone, but some situations warrant more specific investigation. Bone density measurement with DEXA is recommended in guidelines especially for postmenopausal women and older men with risk factors for fragility fracture. Several modern guidelines also emphasize that fracture risk can first be estimated with clinical risk tools, and that DEXA is then used to refine the risk assessment and provide a baseline for follow-up.
You should consider screening if you:
have had a low-energy fracture, such as a wrist, vertebra or hip fracture
are postmenopausal and have multiple risk factors
are over 50 years of age with risk factors for osteoporosis
are using cortisone for a long time
have involuntary weight loss
feel clearly weaker in your legs or arms
have difficulty getting up from a chair, climbing stairs or carrying grocery bags
fall often or feel unsteady
have a chronic illness that affects nutrition, hormones or physical activity
How are the results interpreted – and what can be done if the values are low?
When measuring bone density, T-scores and sometimes Z-scores are often used. T-scores compare bone density with young healthy adults and are mainly used in postmenopausal women and men from the age of 50. Z-scores compare with people of the same age and gender and may be more relevant in younger people. Guidelines emphasize that T-scores from the hip, lower back or in some cases the forearm can be used diagnostically, but that the interpretation must take into account technical and clinical factors.
For muscle mass, there is not the same global simplicity as for osteoporosis diagnostics. Different reference values and indices are used, and therefore DEXA results for muscle mass need to be assessed together with strength and function. This is an important reason why one should not draw too far-reaching conclusions from a single body composition value.
If the examination shows low bone density or suspicion of sarcopenia, the next step is often a combination of:
medical assessment of risk factors and possible underlying diseases
review of diet, especially energy and protein intake
structured strength training
fall prevention and balance exercises
sometimes laboratory tests, such as vitamin D, kidney function, calcium, thyroid tests or testosterone/other hormonal analyses depending on the situation
in some cases drug treatment for osteoporosis
The most important thing in sarcopenia is almost always to improve function, not just numbers. For many patients, it is about regaining enough strength to be able to live independently: getting up from the floor, walking safely outdoors and coping with the stresses of everyday life.
Treatment and prevention – what actually makes a difference
The strongest non-pharmacological measure against sarcopenia is progressive strength training, i.e. resistance training that is gradually increased over time. Research and guidelines show that the combination of exercise and adequate protein intake improves strength, physical function and often muscle mass in older adults and people with sarcopenia.
In practice, this can include:
leg presses, chair squats or sit-to-stand
rowing, pull-ups and upper body presses
balance exercises
walking or other cardio training as a supplement
When it comes to nutrition, modern evidence indicates that older people often need more protein than the minimum level to maintain muscle mass. Many expert reviews indicate that approximately 1.0–1.2 g of protein per kilogram of body weight per day may be reasonable for healthy older people, and that the need is often higher – around 1.2–1.5 g/kg/day – in the event of illness, frailty or established sarcopenia, unless kidney disease or other conditions require individual adaptation.
Lifestyle is also central to the skeleton. Guidelines recommend a nutritious diet, physical activity and measures to reduce the risk of falls. In cases of clearly increased fracture risk, medication may be appropriate, but the basis is still to identify the risk in time and take the right measures before the first or next fracture occurs.
Measuring bone density and muscle mass is therefore not only relevant for those who are already ill. It is also a way of working preventively – to detect changes before they lead to falls, fractures or loss of independence.



