Quick version
Atherosclerosis often begins long before you notice anything, it is small damage to the blood vessels that causes cholesterol and inflammatory cells to be stored in the vessel wall and form plaque. Over time, the vessels can become narrower – but the most dangerous thing is when an unstable plaque ruptures and quickly forms a blood clot, which can lead to a heart attack or stroke.
The most important risk factors you should be aware of are high LDL cholesterol, smoking, high blood pressure, diabetes, obesity and a sedentary lifestyle. Much can be influenced through lifestyle, but sometimes medication is also needed.
Since the disease is often silent for many years, it is important to check your values in time. New guidelines emphasize more individualized risk assessment, where imaging diagnostics such as CT of the heart can also be used to detect early atherosclerosis and prevent serious events.
It's easy to think that a heart attack comes on suddenly, but in reality the process often begins many years earlier – it creeps up silently, without any obvious symptoms. Small changes in the walls of blood vessels can over time develop into atherosclerosis, also known as atherosclerosis, where fat, cholesterol, inflammatory cells and connective tissue build up in the vessel wall. It is only when blood flow becomes too narrow or a plaque ruptures that the disease becomes noticeable, sometimes as angina, stroke or heart attack. That is why knowledge, prevention and early testing are so important.
What happens in atherosclerosis – from fat accumulation to heart attack?
How does atherosclerosis start in the blood vessels?
Atherosclerosis is not just “fat that gets stuck in the vessels”. It is an active biological process in the walls of the arteries that often begins with the innermost layer of the blood vessel, the endothelium, being negatively affected by risk factors such as high LDL cholesterol, smoking, high blood pressure, diabetes, obesity and low physical activity. When the endothelium functions less well, the vessel wall becomes more susceptible to LDL particles entering and remaining in the vessel wall.
LDL is usually called “bad cholesterol”, but it is actually more correct to say that elevated LDL increases the risk of cholesterol being stored where it does not belong. LDL cholesterol can change chemically inside the vessel wall, including through oxidation. The body's immune system then reacts, the white blood cells, especially monocytes, develop into macrophages and take up the changed cholesterol and become so-called foam cells. This is an early step in the formation of plaque itself. Inflammation therefore plays a central role from the very beginning.
Atherosclerosis is not a purely mechanical “recalcification”, but a combination of several factors:
- fat deposition
- chronic low-grade inflammation
- damage or dysfunction in the vessel wall
- the body’s attempt to repair the damage
- later sometimes blood clot formation
It is common for patients to ask the question “Can I have atherosclerosis even if I feel well?”, and the answer is yes. Often, no symptoms appear at all in the early stages. Many people first learn that something is wrong when they develop angina, have a TIA, a stroke or a heart attack.
From fatty streak to plaque – that's why the vessels become narrower
Over time, the early fatty deposits develop into an atherosclerotic plaque. Plaque is not only made up of cholesterol, but also of connective tissue, inflammatory cells and dead cell debris, and sometimes calcium. The body tries to encapsulate the process by forming a fibrous “cap” on top of the plaque. In some cases, the plaque becomes relatively stable and grows slowly. What then happens is that the vessel can gradually become narrower, which reduces blood flow, especially during exertion when the heart or legs need more oxygen.
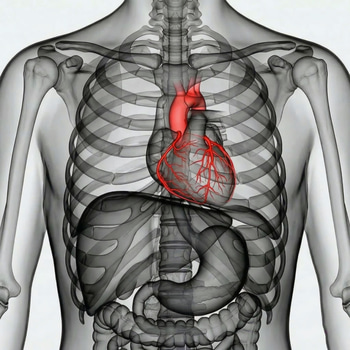
If this occurs in the coronary arteries of the heart, it can cause:
- pressure on the chest during exertion
- shortness of breath
- unusual fatigue
- sometimes radiating discomfort to the arm, back or jaw
If the same process instead occurs in the arteries of the legs, the person may experience pain in the calves when walking, known as claudication. In the carotid arteries, atherosclerosis can increase the risk of TIA and stroke. Atherosclerosis is therefore a systemic disease and not just something that affects the heart.
Therefore, plaques can rupture and cause a heart attack
What often triggers a heart attack is not that a vessel has slowly become a little narrower, but that an unstable plaque ruptures or wears away. When the surface of the plaque is damaged, the blood comes into contact with substances inside the plaque that strongly activate coagulation, and then a blood clot can form very quickly. If the blood clot blocks a coronary artery, the oxygen supply to the heart muscle is cut off - and the result can be a heart attack. The same principle can lead to ischemic stroke in the vessels of the brain.
This explains why a person can sometimes feel relatively well one day and suffer acutely the next. A plaque does not have to be the largest in the vessel to be the most dangerous; the most dangerous plaque may be the most inflammatory and most likely to rupture. Research shows that immune cells, including T cells, contribute to inflammation in plaques and can influence which plaques become unstable and prone to rupture.
The risk factors that drive the process – and what you can influence
The most important modifiable risk factors behind atherosclerosis are well known. The WHO particularly emphasizes tobacco use, unhealthy diet, physical inactivity and harmful alcohol use as central underlying risk behaviors. These often lead to increased blood pressure, increased blood sugar, obesity and elevated blood fats – in other words, the very conditions that drive atherosclerosis.
Some of the most important risk factors to be aware of and prevent are:
- high LDL cholesterol and other unfavorable blood fats
- high blood pressure
- diabetes or prediabetes
- smoking and nicotine exposure
- abdominal obesity and overweight
- physical inactivity
- chronic kidney disease
- old age and heredity
- sleep problems and long-term unfavorable lifestyle
This also means that much can be influenced. Preventive treatment is based on two main tracks: lifestyle habits and medical risk reduction.
Lifestyle habits that reduce risk:
- stop smoking
- regular physical activity
- diet with lots of vegetables, whole grains, legumes, fish and unsaturated fats
- weight loss if overweight
- good sleep and sustainable stress management
- moderate or no alcohol consumption
Medical measures may include:
- treatment of high LDL, which is often done with statins
- blood pressure treatment
- treatment of diabetes
- in some cases additional treatment with other lipid-lowering drugs
- antiplatelet treatment may be appropriate in some patients with established cardiovascular disease
The latest guideline work from ACC/AHA 2026 highlights a more individualized risk assessment, where traditional risk factors are supplemented with biomarkers and so-called risk enhancers. At the same time, the central role of blood lipids, especially LDL cholesterol, in the development of atherosclerotic cardiovascular disease is emphasized. The ESC's updates also emphasize the importance of early and intensive LDL lowering in high-risk patients.
As a complement to these risk models, imaging diagnostics are also highlighted. This applies in particular to the coronary calcium score (CAC), a CT-based method that can detect subclinical atherosclerosis in the coronary arteries of the heart. By visualizing early changes in the vessel wall, the examination can help to better estimate the individual risk and guide decisions about preventive treatment. Here you can read more about the examination CT heart – Calciumscore.
When should you test your values – even without symptoms?
As previously mentioned, atherosclerosis is a condition that is often silent for many years, so testing is particularly valuable before symptoms occur. The WHO also emphasizes that early detection is important so that both important advice and treatment can be initiated in time. It is important for everyone to have insight into their values to minimize the risk of contracting a preventable disease. It is especially wise to check your values if you:
- have a family history of heart attack or stroke
- smoke or have smoked
- have high blood pressure
- are overweight, especially abdominal obesity
- have diabetes, prediabetes or gestational diabetes in the background
- are sedentary
- have had elevated blood lipids in the past
- experience new chest pain, shortness of breath or decreased energy
During a health check it is often particularly relevant to look at:
- total cholesterol, LDL, HDL and triglycerides
- blood sugar and long-term blood sugar
- blood pressure
- weight, BMI and waist measurement
- sometimes additional risk assessment depending on age, symptoms and family history
It is important to bear in mind that a normal everyday life does not exclude risk, many who suffer from early atherosclerosis feel completely healthy. A health check that measures blood fats, blood sugar and other risk markers often makes it possible to detect an unfavorable development in time - before it leads to acute complications.